Rupture of the pectoralis major muscle is a once rare injury that is becoming more common due to increasing numbers of intense weight-training and high-performance athletes. While the diagnosis is usually suspected clinically, assessment of the extent and location of the injury is often limited in the acute setting. With an understanding of the complicated anatomy of the pectoralis major musculotendinous unit, MRI provides the anatomic detail necessary to allow accurate localization and characterization of pectoralis major musculotendinous injuries.
The pectoralis major muscle is a fan shaped muscle with 3 heads originating from clavicular, sternal and abdominal origins. The clavicular head takes origin from the medial one half to two thirds of the clavicle. The upper portion of the sternal head arises from the manubrium and upper body of the sternum and ribs.2-4 The lower portion of the sternal head arises from the distal body of the sternum and ribs.5-6 The abdominal head arises from the external oblique muscle fascia.1 Although indistinguishable by MR, the pectoralis tendon is composed of two laminae: the clavicular lamina and the sternal lamina. The clavicular lamina is composed of fibers from the clavicular head and the upper sternal head fibers with the tendon fibers arising from the clavicular head being most superficial. The distal inserting fibers of the clavicular lamina blend with the distal deltoid inserting fibers. The sternal lamina is composed of the lower sternal and abdominal heads and insert deep and proximal to the clavicular lamina, contributing to the long biceps tendon sheath. The fibers from the abdominal head undergo a 180-degree rotation before inserting on the humerus. Thus the tendon fibers from the abdominal head are most superior in their insertion onto the lateral aspect of the bicipital groove
The multiple muscle head origins and crossing pattern of insertion allow the pectoralis major muscle to exert a wide range of actions on the humerus. Depending on the position of the humerus, the pectoralis major muscle can adduct, flex, and internally rotate the humerus against a stable thorax. Against a fixed humerus, the pectoralis muscle acts as a climbing muscle, pulling the thorax upward. It is also an accessory muscle of respiration when the shoulders are fixed in an elevated position.
 A coronal oblique T1-weighted image demonstrates normal anatomy of the pectoralis major muscle. The pectoralis muscle is made up of three heads: the clavicular head (CH), the sternal head (SH), and the abdominal head (AH). The clavicular head fibers (blue) combine with the superior sternal head fibers (green) to form the clavicular head lamina. The lower sternal head fibers (red) and abdominal head fibers (yellow) form the sternal lamina and insert deep to the clavicular head lamina with the abdominal head fibers (yellow) inserting most superiorly. The cephalic vein (arrow) is a reliable landmark separating the anterior deltoid (D) from the clavicular head (H) of the pectoralis major. The humeral head (HH) and Biceps muscle (B) are also indicated.
A coronal oblique T1-weighted image demonstrates normal anatomy of the pectoralis major muscle. The pectoralis muscle is made up of three heads: the clavicular head (CH), the sternal head (SH), and the abdominal head (AH). The clavicular head fibers (blue) combine with the superior sternal head fibers (green) to form the clavicular head lamina. The lower sternal head fibers (red) and abdominal head fibers (yellow) form the sternal lamina and insert deep to the clavicular head lamina with the abdominal head fibers (yellow) inserting most superiorly. The cephalic vein (arrow) is a reliable landmark separating the anterior deltoid (D) from the clavicular head (H) of the pectoralis major. The humeral head (HH) and Biceps muscle (B) are also indicated.
The pectoralis tendon is best seen on axial T1 and T2-weighted images as a curvilinear low-signal band inserting onto the lateral ridge of the bicipital groove of the humerus. The superior-most inserting fibers can be identified curving anterior to the biceps tendon at the approximate level of the quadrilateral space (D).3 The tendon length is variable ranging from 5 to 15 mm and the fibers insert over a cephalocaudal distance of 4-6 cm. The distal extent of tendon insertion is typically seen just proximal to the deltoid tubercle.3 The pectoralis major muscle is the most superficial muscle group along the superior chest wall, separated from the anterior deltoid by the deltopectoral groove, which contains the cephalic vein(C).
 Axial T1-weighted image at the level of the quadrilateral space (Q) demonstrates the pectoralis major tendon (arrow) curving anterior to the coracobrachialis and short biceps muscles (CB) to insert on the lateral ridge of the biceps groove. The clavicular head of the pectoralis major muscle (CH) and the deltoid muscle (D) are also identified.
Axial T1-weighted image at the level of the quadrilateral space (Q) demonstrates the pectoralis major tendon (arrow) curving anterior to the coracobrachialis and short biceps muscles (CB) to insert on the lateral ridge of the biceps groove. The clavicular head of the pectoralis major muscle (CH) and the deltoid muscle (D) are also identified.
MRI IMAGING PALNES FOR PECTORALIS MUSCLE
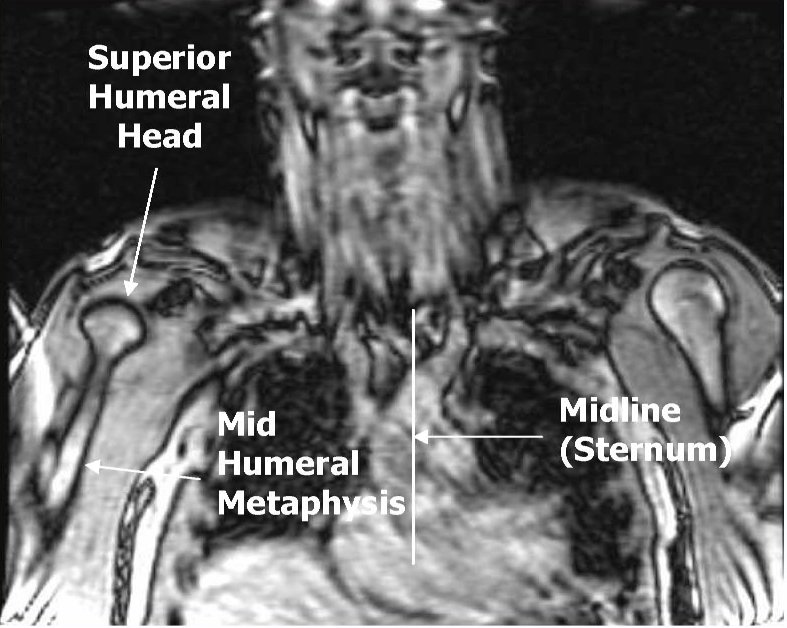
Axial Plane: Scan from superior humeral head through the xyphoid process. The field of view should include the sternum medially, and the humeral shaft laterally.

Coronal Plane: Prescribe a plane parallel to the line from sternum through anterior humerus. Scan from skin through posterior humeral head. Field of view should include the sternum and humerus.


Sagittal Plane: Prescribe plane perpendicular to coronal plane. Scan From sternum through lateral aspect of humerus

|
Image Plane
|
Sequence
|
FOV (cm)
|
TE / (TR)
|
Slice / gap
|
|
Axial
|
T1
|
20-22
|
|
|
|
Axial
|
T2 Fat Sat
|
20-22
|
60
|
|
|
Coronal
|
T1
|
20-22
|
|
|
|
Coronal
|
STIR
|
20-22
|
|
|
|
Sagittal
|
PD Fat Sat
|
20
|
60
|
|
Pectoralis Tear PROTOCOL
- Axial and coronal Images should include sternum and humeral head.
- Positioning the patient prone will reduce breathing motion artifacts.
- Phase encode should be in the transverse direction on axial images, craniocaudal on sagittal images.
Injury Mechanism and Physical Examination
Injury of the pectoralis major tendon or musculotendinous junction most commonly occurs when the muscle is under extreme tension with application of additional forceful stretching. These injuries are most often encountered in weight lifters, with the injury occurring almost exclusively during bench-press exercise. Pectoralis major tendon injuries are also seen in football, waterskiing, and wrestling.
The patient typically presents after experiencing a "pop" following excessive muscle tension or after a direct blow to the shoulder while the arm is in abduction and extension. Ecchymosis and swelling are seen in the axilla and upper arm with asymmetry of the pectoralis musculature. In the acute setting, marked edema, pain, and decreased range of motion may hinder the clinical assessment of the extent and location of the injury.
MRI offers multiplanar imaging and fluid sensitive sequences that are ideal for evaluating acute pectoralis major muscle and tendon injuries. Fluid sensitive sequences are valuable for detecting the site of injury, demonstrating edema and hemorrhage in the muscle, tendon and in the surrounding soft tissues. The multiplanar capabilities of MRI allow optimal depiction of the portions of the pectoralis major muscle and tendon involved.
Incomplete ruptures of the pectoralis major are most common and typically occur at the musculotendinous junction or muscle belly of the sternal head.4 Edema and hemorrhage are seen at the site of the musculotendinous tear. The muscle may be retracted, but the inserting pectoralis major tendon fibers remain intact without associated hemorrhage or edema (E).
 Axial T2-weighted fat-suppressed image demonstrates a musculotendinous rupture (arrow) of the sternal head (SH) which is mildly retracted. The pectoralis major tendon is normal at its humeral insertion (arrowhead). The clavicular head (CH) demonstrates mild edema at this level, indicating a muscle strain. The asterisk indicates the cephalic vein. The deltoid muscle (D) and coracobrachialis and short biceps muscles (CB) are indicated
Axial T2-weighted fat-suppressed image demonstrates a musculotendinous rupture (arrow) of the sternal head (SH) which is mildly retracted. The pectoralis major tendon is normal at its humeral insertion (arrowhead). The clavicular head (CH) demonstrates mild edema at this level, indicating a muscle strain. The asterisk indicates the cephalic vein. The deltoid muscle (D) and coracobrachialis and short biceps muscles (CB) are indicated
Complete ruptures occur most commonly at the distal tendon or its insertion.5 Hemorrhage and edema are seen anterior to the humerus without visualization of the inserting pectoralis major tendon fibers. The biceps tendon may be slightly displaced from its normal location anterior to the humerus because of associated biceps sheath injury and periosteal hemorrhage and edema (F)
. Axial fat-suppressed proton-density weighted image at the level of the quadrilateral space (Q) demonstrates hemorrhage and edema anterior to the humerus (black arrow), representing periosteal stripping at the site of tendon avulsion. The pectoralis major muscle tendon (white arrow) is mildly retracted. With disruption of the pectoralis major tendon insertion the long biceps tendon (arrowhead) is mildly displaced from the biceps groove.
In patients with pectoralis major ruptures, coronal oblique images along the plane of the muscle and tendon are helpful in establishing which portions of the pectoralis major muscle are involved (G).
 A Coronal oblique T2-weighted image demonstrates a rupture of the sternal head (SH) of the pectoralis major at the musculotendinous junction (arrow). The clavicular head (CH) is intact and can be identified as separate from the deltoid (D) by the cephalic vein (arrowhead). The abdominal head (AH) is also spared in this particular injury.
A Coronal oblique T2-weighted image demonstrates a rupture of the sternal head (SH) of the pectoralis major at the musculotendinous junction (arrow). The clavicular head (CH) is intact and can be identified as separate from the deltoid (D) by the cephalic vein (arrowhead). The abdominal head (AH) is also spared in this particular injury.
Isolated pectoralis major intramuscular tears may be seen as a result of a bench-press injury, but they more frequently occur from a direct blow to the muscle. Intramuscular increased signal on fluid sensitive sequences easily confirms this injury, and is effective in evaluating its extent (H

