



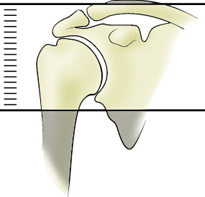
AXIAL REFERENCE LINES
Axial Imaging Plane
Prescribe plane parallel to humeral shaft. Cover from AC joint through proximal humeral diaphysis.
Use coronal LOC and plane is straight horizontal (IF THE SHOULDER IS MARKEDLY ANGLED, YOU CAN ANGLE THE AXIAL IMAGES PERPENDICULAR TO THE GLENOHUMERAL JOINT)
- Cover from top of AC joint down and try to cover to the inferior portion of
the glenohumeral joint axillary pouch
- No Sat Band


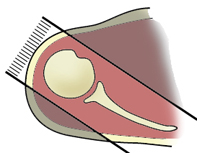
CORONAL REFERENCE LINES
Coronal Imaging Plane Prescribe coronal plane off of axial images parallel to supraspinatus muscle
Use axial sequence to orient the plane along the
supraspinatus tendon
- If the supraspinatus tendon is not well seen, you can either use the teres
minor tendon or the glenohumeral joint
- Cover from anterior portion of coracoid process to 1 slice posterior to the
humeral head.
- Oblique Sat band over chest




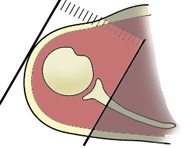
SAGITAL REFERENCE LINES
Sagittal Imaging Plane Prescribe sagittal plane off axial images with line parallel to bony glenoid. Image from bony glenoid through deltoid muscle.
Perpendicular to Coronal sequence
- Angle approximately parallel to GH joint on the Cor T2 sequence (use
Glenoid articulating surface to angle)
Cover from 1 slice out of humeral head to as far medial as slices allow
- Oblique Sat band over chest
- Oblique Sat band over chest
- Cover from 1 slice out of humeral head to as far medial as the slices go
(to approx. the medial portion of the coracoid process)










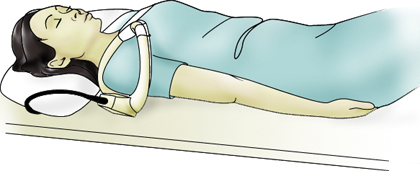
Imaging the shoulder is optimal with a dedicated shoulder coil and careful patient positioning in external rotation with the shoulder as close as reasonably possible to the center of the magnet. Axial proton density, coronal oblique T2 fat sat and proton density, and sagittal oblique T2 provide an assessment of the rotator cuff, biceps, deltoid, acromio-clavicular joint, the gleno-humeral joint and surrounding large structures. If a labral injure is suspected, the optional fat sat gradient echo sequence (series 6) may be helpful or it may be necessary to bring the patient back for an MR shoulder arthrogram with intra-articular injection of dilute gadolinium.
Routine shoulder protocols are the most variable, but most include
SHOULDER MRI SEQUENCES
AX PD TSE SPIR (3 mm slices)
AX PD TSE SPIR (3 mm slices) Particularly useful for assessment of the long head of the biceps tendon and subscapularis tendon. Glenohumeral ligaments, glenoid labrum and acramioclavicular joint are also assessed.
Coronal Fat-Sat PD spin echo (SE) Supraspinatus tendons and acromioclavicular joint are assessed. Superior labrum is also visualized well on this sequence.
COR Oblique T2 TSE SPIR Particularly useful to determine if the signal abnormalities in the supraspinatus tendons and superior labrum is truly due to degeneration or tear, and also to see if there is any fluid in the subacromian and subdeltoid bursa (which would be due to bursitis or rotator cuff tear). Bone edema like abnormalities also easily appreciated.
SAG T1 SE SPIR T1 sequence is useful to assess the bone marrow. Bone marrow replacing conditions are best evaluated with this sequence. Supraspinatus tendon impingement is also easily appreciated.
Sagittal Fat-Sat PD spin echo (SE) Useful to confirm findings appreciated on coronal plane and also useful for further assessment of the biceps tendon and its superior labral attachment.
For labral pathology 2 mm cuts through the glenohumeral joint
Positioning: supine with arm at side and palm facing up. It is useful to tuck the hand under the hip to help keep the shoulder motionless. It is important to shift the patient to one side of the magnet so the shoulder being imaged is closer to the center, “sweet spot” of the magnet. This is especially helpful for fat saturation. Place a vitamin E capsule at the site of any mass or symptoms. A wide strap over the shoulder cinched down tight to the table can help reduce shoulder motion during breathing.
- Try to have shoulder neutral (external rotation is fine)
- Try to limit superior or inferior positioning of shoulder when compared to
the chest (IF THE SHOULDER IS MARKEDLY ANGLED, YOU CAN ANGLE THE
AXIAL IMAGES PERPENDICULAR TO THE GLENOHUMERAL JOINT)
- Try to place shoulder as close to isocenter in the bore of the magnet
- Place a sponge at the elbow and one supporting the hand and strap the
- Large 4 channel flex coil for larger patient (make certain that coverage
has enough signal for the AC joint)
- Body matrix coil for an extremely large patient
The sequence evaluates the acromial arch, including acromial inferior cortex, acromioclavicular joint, and coraco-acromioligament.














 CORONAL PD FSE
CORONAL PD FSE CORONAL T2 FAT SAT FSE
CORONAL T2 FAT SAT FSE SAG PD FAT SUPPRESSED FSE
SAG PD FAT SUPPRESSED FSE SAG PD FSE
SAG PD FSE AXIAL PD FAT SAT FSE
AXIAL PD FAT SAT FSE AXIAL GRADIENT
AXIAL GRADIENT
 Axial T1 fat saturated
Axial T1 fat saturated Sagital oblique T1 fat saturation
Sagital oblique T1 fat saturation ABER T1 (abduction external rotation)
ABER T1 (abduction external rotation)