|
|
|
 |
|
STERNO CLAVICULAR JOINTS ANATOMY & MRI PROTOCOL |
|
|
|
|
|
|
|
|
|
|
|
The sternum and sternoclavicular joints are difficult to evaluate with plain radiographs. The value of CT in assessing lesions of the sternum and sternoclavicular joints has been well documented, but the potential role of MRI has not been emphasized. We present the MRI techniques, normal appearances and a spectrum of abnormalities, and emphasize the role of MRI as a useful radiological investigation for the sternum and sternoclavicular joints.

Breath-hold images were obtained in threeorthogonal planes, coronal, sagittal and axial,using a general purpose body array coil on a1.5 T Siemens Vision scanner (Siemens, Erlangen,Germany). Coronal images were obtained in two oblique planes, one parallel to the manubrium and the other parallel to the body of the sternum.
Both T1 and T2 weighted images were acquired. Short tau inversion recovery (STIR) or fat suppressed T2 weighted images were acquired in the optimal plane to depict the pathology. Respiratory gating was required for STIR sequences only
Normal appearances
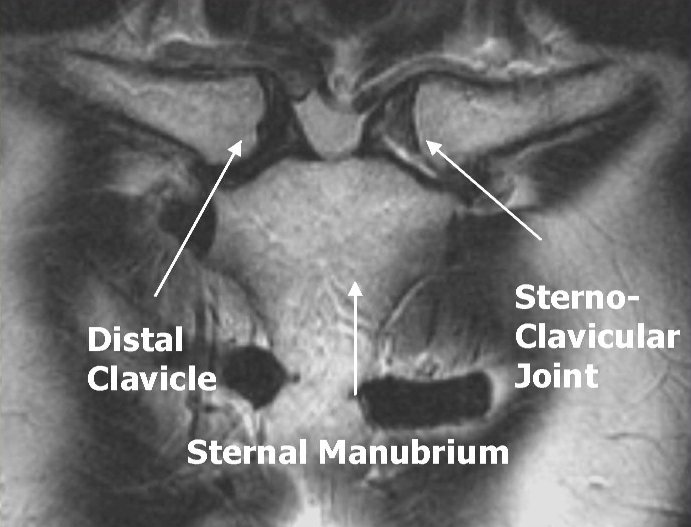
The sternum is optimally demonstrated in the sagittal plane with clear delineation of the manubrium, the body of the sternum and the xiphoid process. The outer cortex and central marrow are well seen (Figure 1 ). Coronal images are obtained in two planes for clear views of the manubrium and body of the sternum as they are angulated at the manubriosternal junction. The axial images provide additional information, particularly in the evaluation of congenital chest wall deformities. ). Coronal images are obtained in two planes for clear views of the manubrium and body of the sternum as they are angulated at the manubriosternal junction. The axial images provide additional information, particularly in the evaluation of congenital chest wall deformities.
The sternum is a flat bone, slightly convex anteriorly and concave posteriorly. It consists of three parts: the manubrium, body, and xiphoid process. It tends to narrow at the junction between the body and manubrium and the junction between the body and the xiphoid process
 Normal sternal anatomy. Normal sternal anatomy.
Coronal reformatted image from chest CT shows the three parts of the sternum—the manubrium (M), sternal body (B), and xiphoid process (X)—as well as the clavicles (C), internal mammary arteries (arrowheads), and anterior (red) and posterior (blue) muscular insertions, including the origins of the sternocleidomastoideus (1), subclavius (2), and pectoralis major (3); attachments of the sternohyoideus (4) and sternothyroideus (5); origin of the transversus thoracis (6); and attachments of the small part of the rectus abdominis (7) and fibers of the diaphragm and transversus thoracis (8).
The manubrium is the broadest portion of the sternum, and the farthest cephalad. It has a superior central notch (suprasternal or jugular notch) and two lateral fossae (clavicular notches) that articulate with the clavicles. The manubrium also articulates with the first and second ribs and the body of the sternum. Several muscles (eg, sternocleidomastoideus, sternohyoideus, and sternothyroideus) are attached to its anterior surface .
The body of the sternum is flat, with an irregular anterior surface. Superiorly, it articulates with the manubrium at the manubriosternal joint (also called the sternal angle or symphysis). Inferiorly, it articulates with the xiphoid process. The lateral borders of the sternum articulate with the second through seventh ribs. The pectoralis major muscles insert on its anterior surface. The angle between the body and the manubrium (sternal angle) is an important clinical landmark because it demonstrates the site of articulation with the second rib .
The xiphoid process (from the Greek word xiphos, meaning “straight sword”) is a thin and elongated bone that is subject to many variations. It is cartilaginous early in life and may become completely ossified and fused to the sternal body in old age .
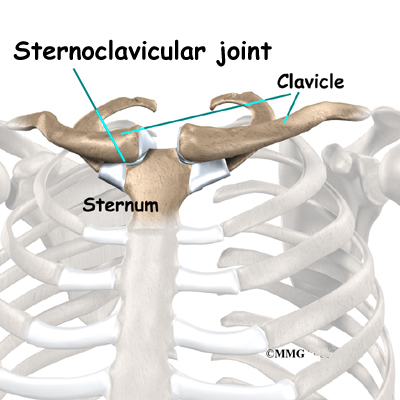
The sternoclavicular joint is a synovial joint that connects the axial skeleton and the upper extremity and is involved in the movement of the upper extremities The major components of the sternoclavicular joint include the anterior sternoclavicular ligament, interclavicular ligament, costoclavicular ligament, articular disk, and articular cavities .
Computed tomography (CT) is the modality of choice to evaluate anatomic detail as well as pathologic conditions of the sternum, sternoclavicular joints, and adjacent soft tissues .
CT allows differentiation of the cortex from the medulla; depicts normal spiculations and pits, among other variants; and allows normal variants to be differentiated from pathologic abnormalities . Although the appearance of the cortex is usually sharp, the lower two-thirds of the posterior margin of the manubrium may be ill defined and occasionally absent (a normal variant). The xiphoid appendage may be absent, occur with structural variations (eg, a double- or triple-ended configuration), and contain clumpy or irregular calcifications . The two sternoclavicular joints are usually symmetric. Each is divided into two compartments by a fibrocartilaginous disk. Gas within the joint space, also known as the vacuum phenomenon, is frequently identified at CT or conventional radiography and should not be mistaken for an abnormal finding
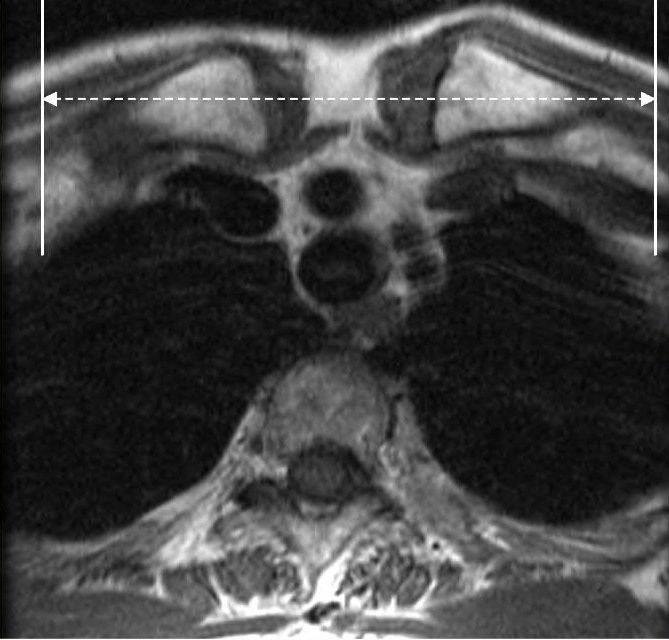
Magnetic resonance (MR) imaging is of great value as a secondary modality. It can help clarify CT findings and can provide additional information about the bone marrow and soft tissues adjacent to the sternum . At MR imaging, the sternal anatomy is best depicted with T1-weighted spin-echo pulse sequences. The coronal plane displays the articular surfaces, as well as the intraarticular disk; the sagittal plane is useful for depicting the costoclavicular ligament; and the axial plane best delineates the anterior and posterior parts of the sternoclavicular joint capsule and the anterior and posterior sternoclavicular ligaments . Normal findings that should not be mistaken for disease include small amounts of joint fluid, nonfatty bone marrow, and poorly defined cortical margins
MRI SERNOCLVICULAR JOINT PROTOCOL
|
Image Plane
|
Sequence
|
FOV (cm)
|
TE / (TR)
|
Slice / gap
|
|
Axial
|
T1
|
20
|
|
|
|
Axial
|
T2 Fat Sat
|
20
|
60-80
|
|
|
Coronal
|
T1
|
20
|
|
|
|
Coronal
|
STIR
|
20
|
|
|
|
Sagittal
|
T2 Fat Sat
|
20
|
60-80
|
|
Axial Plane: Center on Sternum on coronal scout and prescribe plane perpendicular to line through sternum. Scan through SC joint.
Coronal Plane: Prescribe perpendicular to SC join. Scan through both clavicle heads
 
Sagittal Plane: Prescribe plane with line that touches the anterior cortex of the sternum and clavicle heads. Scan through both SC joints.
|
The sternoclavicular articulation is a double arthrodial joint. The parts entering into its formation are the sternal end of the clavicle, the upper and lateral part of the manubrium sterni, and the cartilage of the first rib. The articular surface of the clavicle is much larger than that of the sternum, and is invested with a layer of cartilage, which is considerably thicker than that on the latter bone. The ligaments of this joint are:
|
|
|
|
The Articular Capsule.
|
|
The Interclavicular.
|
|
The Anterior Sternoclavicular.
|
|
The Costoclavicular.
|
|
The Posterior Sternoclavicular.
|
|
The Articular Disk.
|
|
| |
|
The Articular Capsule (capsula articularis; capsular ligament).—The articular capsule surrounds the articulation and varies in thickness and strength. In front and behind it is of considerable thickness, and forms the anterior and posterior sternoclavicular ligaments; but above, and especially below, it is thin and partakes more of the character of areolar than of true fibrous tissue.
|
|
| |
|
The Anterior Sternoclavicular Ligament (ligamentum sternoclaviculare anterior).—The anterior sternoclavicular ligament is a broad band of fibers, covering the anterior surface of the articulation; it is attached above to the upper and front part of the sternal end of the clavicle, and, passing obliquely downward and medialward, is attached below to the front of the upper part of the manubrium sterni. This ligament is covered by the sternal portion of the Sternocleidomastoideus and the integument; behind, it is in relation with the capsule, the articular disk, and the two synovial membranes.
|
|
| |
|
The Posterior Sternoclavicular Ligament (ligamentum sternoclaviculare posterius).—The posterior sternoclavicular ligament is a similar band of fibers, covering the posterior surface of the articulation; it is attached above to the upper and backpart of the sternal end of the clavicle, and, passing obliquely downward and medialward, is fixed below to the back of the upper part of the manubrium sterni. It is in relation, in front, with the articular disk and synovial membranes; behind, with the Sternohyoideus and Sternothyreoideus.
|
|
| |
|
The Interclavicular Ligament (ligamentum interclaviculare).—This ligament is a flattened band, which varies considerably in form and size in different individuals, it passes in a curved direction from the upper part of the sternal end of one clavicle to that of the other, and is also attached to the upper margin of the sternum. It is in relation, in front, with the integument and Sternocleidomastoidei; behind, with the Sternothyreoidei.
|
|
| |
|
The Costoclavicular Ligament (ligamentum costoclaviculare; rhomboid ligament).—This ligament is short, flat, strong, and rhomboid in form. Attached below to the upper and medial part of the cartilage of the first rib, it ascends obliquely backward and lateralward, and is fixed above to the costal tuberosity on the under surface of the clavicle. It is in relation, in front, with the tendon of origin of the Subclavius; behind, with the subclavian vein.
|
|
|
|
|
Sternoclavicular articulation. Anterior view.
|
| |
| |
|
The Articular Disk (discus articularis).—The articular disk is flat and nearly circular, interposed between the articulating surfaces of the sternum and clavicle. It is attached, above, to the upper and posterior border of the articular surface of the clavicle;below, to the cartilage of the first rib, near its junction with the sternum; and by its circumference to the interclavicular and anterior and posterior sternoclavicular ligaments. It is thicker at the circumference, especially its upper and back part, than at its center. It divides the joint into two cavities, each of which is furnished with a synovial membrane.
|
|
| |
|
Synovial Membranes.—Of the two synovial membranes found in this articulation, the lateral is reflected from the sternal end of the clavicle, over the adjacent surface of the articular disk, and around the margin of the facet on the cartilage of the first rib; the medial is attached to the margin of the articular surface of the sternum and clothes the adjacent surface of the articular disk; the latter is the larger of the two.
|
|
| |
|
Movements.—This articulation admits of a limited amount of motion in nearly every direction—upward, downward, backward, forward, as well as circumduction. When these movements take place in the joint, the clavicle in its motion carries the scapula with it, this bone gliding on the outer surface of the chest. This joint therefore forms the center from which all movements of the supporting arch of the shoulder originate, and is the only point of articulation of the shoulder girdle with the trunk. The movements attendant on elevation and depression of the shoulder take place between the clavicle and the articular disk, the bone rotating upon the ligament on an axis drawn from before backward through its own articular facet; when the shoulder is moved forward and backward, the clavicle, with the articular disk rolls to and fro on the articular surface of the sternum, revolving, with a sliding movement, around an axis drawn nearly vertically through the sternum; in the circumduction of the shoulder, which is compounded of these two movements, the clavicle revolves upon the articular disk and the latter, with the clavicle, rolls upon the sternum. Elevation of the shoulder is limited principally by the costoclavicular ligament; depression, by the interclavicular ligament and articular disk. The muscles which raise the shoulder are the upper fibers of the Trapezius, the Levator scapulæ, and the clavicular head of the Sternocleidomastoideus, assisted to a certain extent by the Rhomboidei, which pull the vertebral border of the scapula backward and upward and so raise the shoulder. The depression of the shoulder is principally effected by gravity assisted by the Subclavius, Pectoralis minor and lower fibers of the Trapezius. The shoulder is drawn backward by the Rhomboidei and the middle and lower fibers of the Trapezius, and forward by the Serratus anterior and Pectoralis minor.
|
|
|
|
|
|
|
Today, there have been 1 visitors (5 hits) on this page! |